What is C-CDA?

A document to be used in the exchange of patient records is the Consolidated CDA Document (CCDA), an XML file that is described in the HITECH Act's "Meaningful Use" (MU) section. Every MU-certified EHR is capable of producing, sending, receiving, and ingesting CCDA records. This makes it a very strong standard for exchanging longitudinal and episodic care records.
The XML data is simple to use in computing because it has defined fields and codes, unlike other formats like PDFs or faxes.
What’s Contained Within a C-CDA Document?

XML is generally used to express C-CDA documents. They could have organized the data like a list of prescribed medications. They excel at gathering unstructured data, such as pictures. In general, C-CDA is read-only (although the information can be parsed and uploaded elsewhere with some effort). It's a collection of templates that can include data across a range of periods and medical histories.
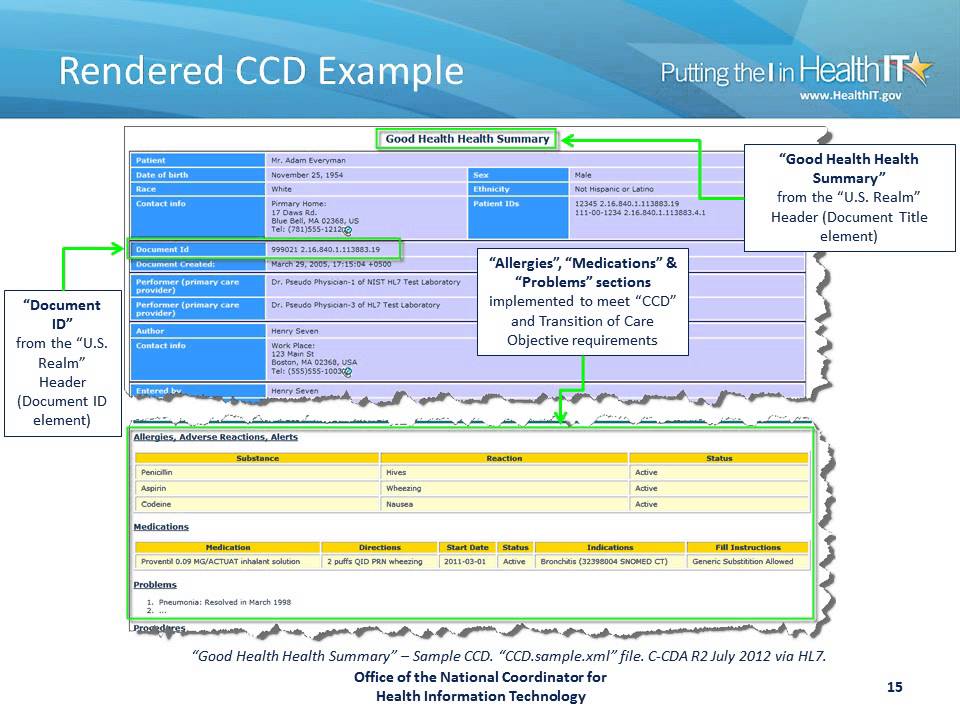
The Continuity of Care Document is another accomplishment of C-CDA (CCD). In C-CDA format, CCDs are documents that provide a snapshot of a patient's medical history.
In actuality, a lot of CDA and C-CDA documents have a narrow scope. For particular use scenarios, the CDA contains a tonne of documents.
A discharge summary, for example, only includes details on a patient's discharge from care. Although the communication transport mechanism is not stated in the standard, a hierarchy of specifications is used to describe the communication mechanisms for clinical papers. IHE International laid the groundwork for the networks with which Particle communicates.
In some ways, C-CDA is a victim of its success. Older CCDs can be quite long, necessitating the use of a technology like Particle's data translation platform to translate the information from CDA to FHIR so that it can be searched more programmatically.
What is CDA?
What is C-CDA consolidating if that is the case? Clinical Document Architecture (CDA), a markup standard for electronic clinical records that was originally published in 2000, was a step in the direction of interoperability. Similar to C-CDA papers, CDA documents are information-containment templates that use XML encoding, which gave them more freedom than the era's strict rules. CDA may use classes, relationships, and inheritance because it is object-oriented.
Common elements or templates can be found in various CDA texts. Continuity of Care Documents, History & Physical, and Consultation Notes all use the same Family History Form. The majority of medical record requirements can be satisfied by CDA thanks to its standard building blocks.
Furthermore, CDA documents incorporate a common feature of other data formats today: a subset of agreed-upon standard medical words. This means that CDA documents are semantically interoperable.
Many papers in the wild fall short of the criteria for CDA, which calls for them to be both machine- and human-readable.
Over time, CDA gained a reputation for having a wide range of variations, which made it challenging to exchange papers written in this style. It was challenging to gain the benefits of potential enhancements since different standards bodies had divergent views on the CDA format. By 2012, various CDA versions, including HL7 CDA, IHE, HITSP, and others, had been incorporated into C-CDA.
What Can Be Found in A CCD Document?
To assist handoffs from one physician to another, continuity of care documents (CCDs) is employed. They record what the health standards group HL7 refers to as a "snapshot in time"— a uniform summary of the pertinent clinical data for a particular patient. CCDs are made to transfer this data from one provider to another without any loss of significance, even though clinician notes can occasionally be vague.
Constraints (or templates) from other CDA documents are used to create CCDs to maximize compatibility. Fields like "must be present in a CCD that satisfies federal Meaningful Use guidelines".
- Demographic information
- An important sign (height, weight, blood pressure, BMI)
- The name and office contact information of the referring or transitioning provider.
- The patient's care team: The team consists of their primary care physician or another approved medical expert, as well as any other known members.
- The basis for the referral
- Diagnosis of the encounter
- A list of current issues
- Laboratory test results, a list of the medications being used at the time, a list of all allergies and intolerances, and a social history
- The management procedures for the patient's various ailments are specified in the care plan field. The treatment plan must include the issue or point of attention, the target or intended outcome, and any directions the doctor has given the patient.
These fields may not always be completely filled out. Particle assists users in combining CCDs from many sources to produce a more thorough patient overview.
Limitations of C-CDA
It's common knowledge among developers that C-CDA is challenging to use. In reality, the majority of EHRs don't store data in CDA or C-CDA format. Some formats were created to facilitate record sharing rather than to store data. When requested, EHRs often transform data into C-CDA documents, which causes compatibility problems.
C-CDA documents can be lengthy—they occasionally top 200 pages. It is challenging to programmatically search within documents; this must be done on the client side. Under the C-CDA paradigm, for instance, you can't just request a patient's medications from the EMR server; you have to obtain all records and then try to separate the crucial data by hand. The C-CDA standard is becoming obsolete due to its inability to satisfy the requirements of contemporary digital health platforms, but Particle's API circumvents this issue by converting from C-CDA to FHIR.
FHIR, A Next Generation Standard, replaces C-CDA
FHIR, a more recent standard, has gained popularity in reaction to C-drawbacks. CDA's Without downloading a whole health record, FHIR also makes it simpler to choose and query particular data pieces, such as a list of medications. C-CDA is less suited to the needs of contemporary digital health since it necessitates additional procedures to connect data with digital health infrastructure.
The preferred format for implementing new healthcare data is typically FHIR. FHIR is necessary for the upcoming wave of national interoperability programmes, much like C-CDA was widely adopted as a result of federal interoperability policy. The Particle API enables healthcare organisations to look up patient information that has been prepared and correctly mapped to FHIR-based resources.
Important legacy of C-CDA
C-CDA normalised the format of data exports from EHRs. This opened the door for more sophisticated interoperability standards. You could claim that it's a successful illustration of healthcare's digital revolution toward full interoperability, as all American EHRs are required to output C-CDA data.
It seems obvious that C-CDA will endure. C-CDA will still be a part of your ABCs if you work in health IT, even if it is gradually being phased out!
Subscribe to our Blogs
Contact Us